Bacteriology Board Review
March 29, 2018
69-year-old woman with pneumatosis of colon
March 30, 2018
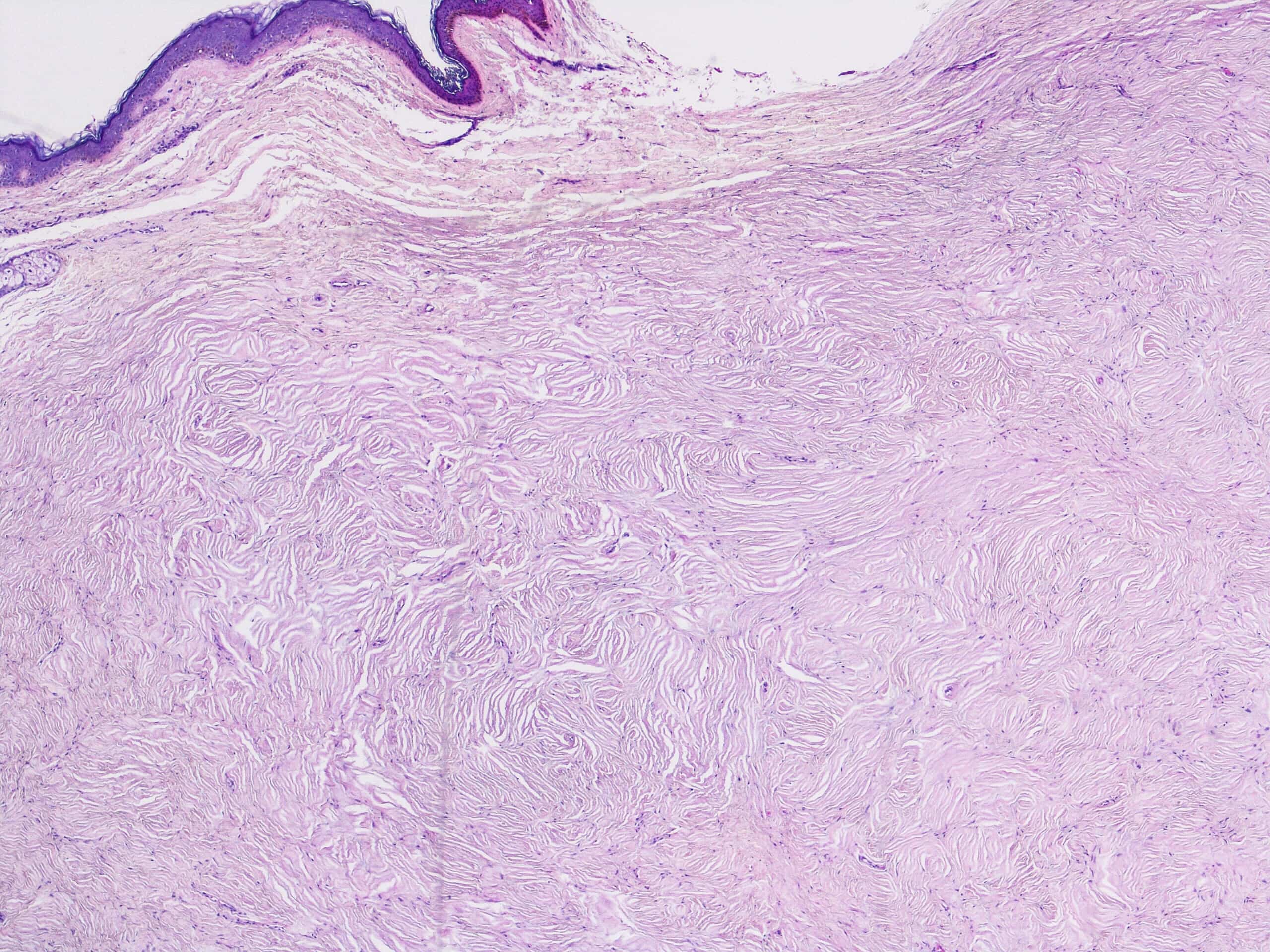
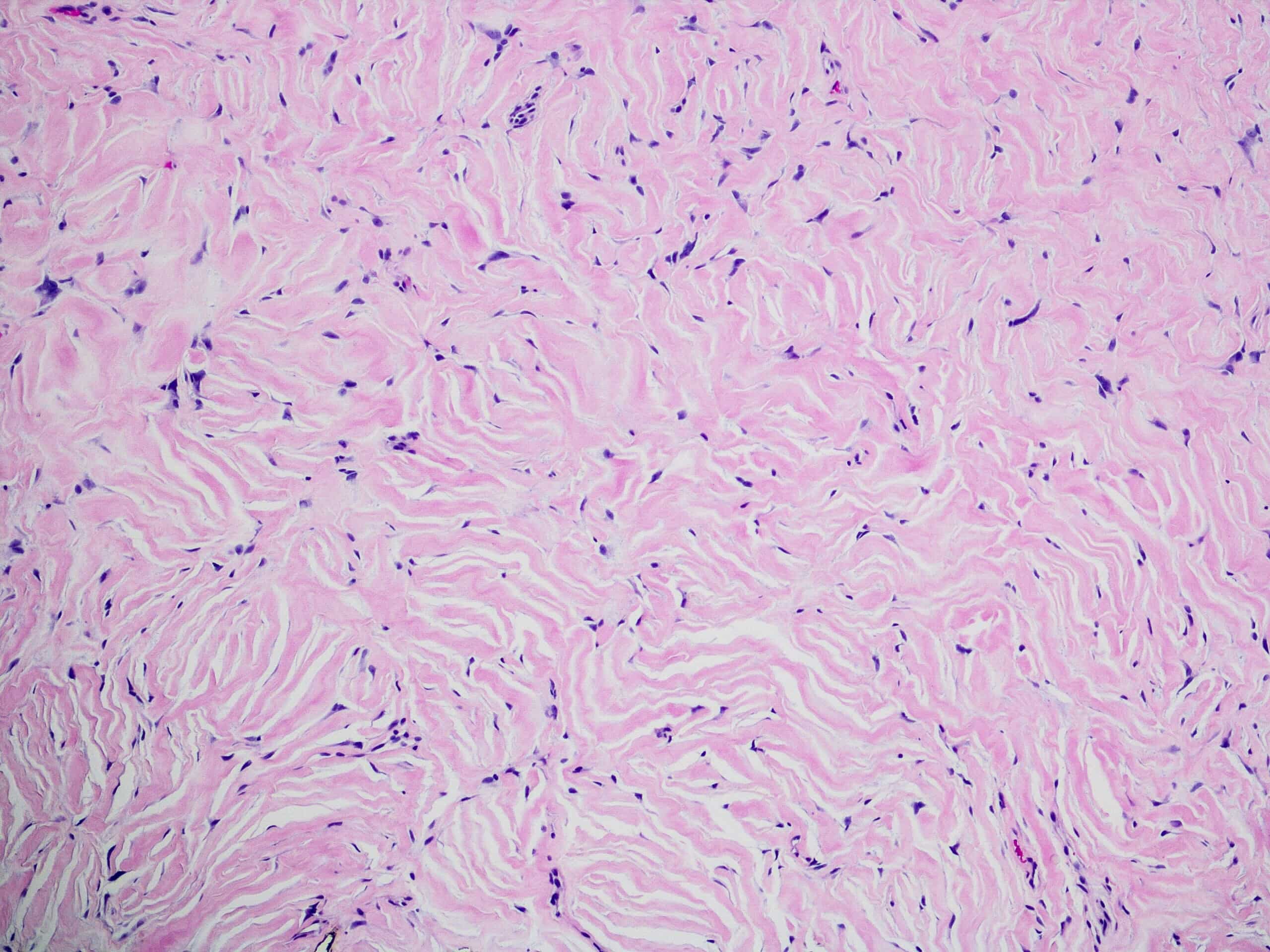
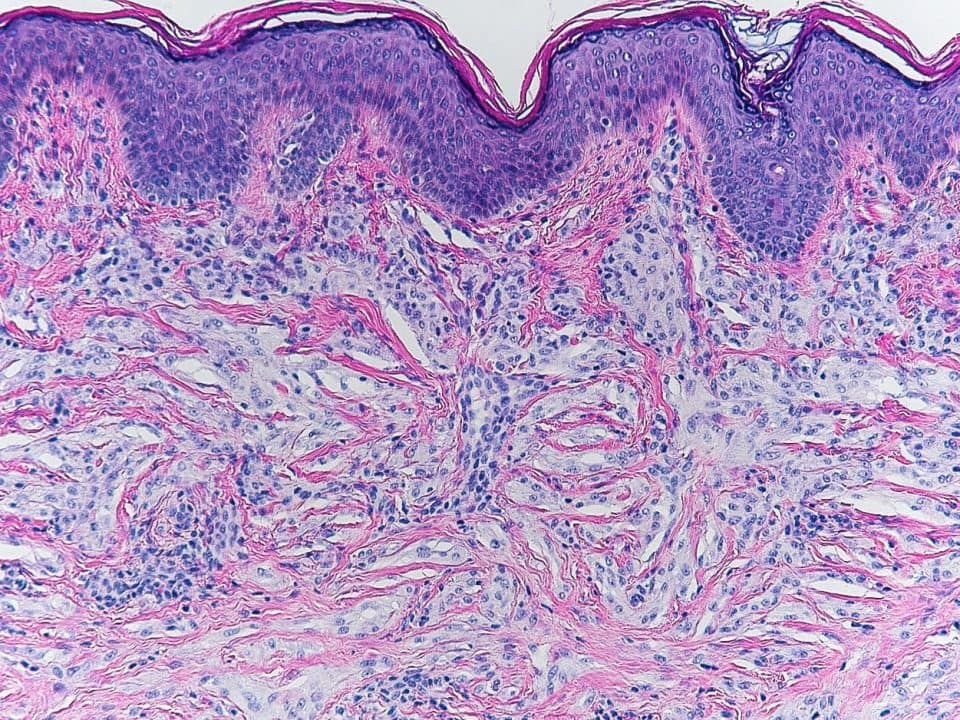
Giant cell collagenoma was first described by Rudolph et al in 1998(1). It is an uncommonly encountered benign dermal neoplasm that has stromal changes reminiscent of storiform collagenoma. Circumscribed storiform collagenoma is also known as sclerotic fibroma or hypocellular fibroma. It was first described as a whorled fibroma by Weary et al in 1972 in the context of patients with multiple hamartomas or Cowden’s syndrome(2). Figure 1 shows a classic hypocellular whorled sclerotic dermal proliferation of collagen bundles underneath a thinned epidermis in a patient with known Cowden’s syndrome. Figure 2 shows 100x magnification of the whorled collagen bundles pattern, which is often called a plywood pattern because of its resemblance to plywood.

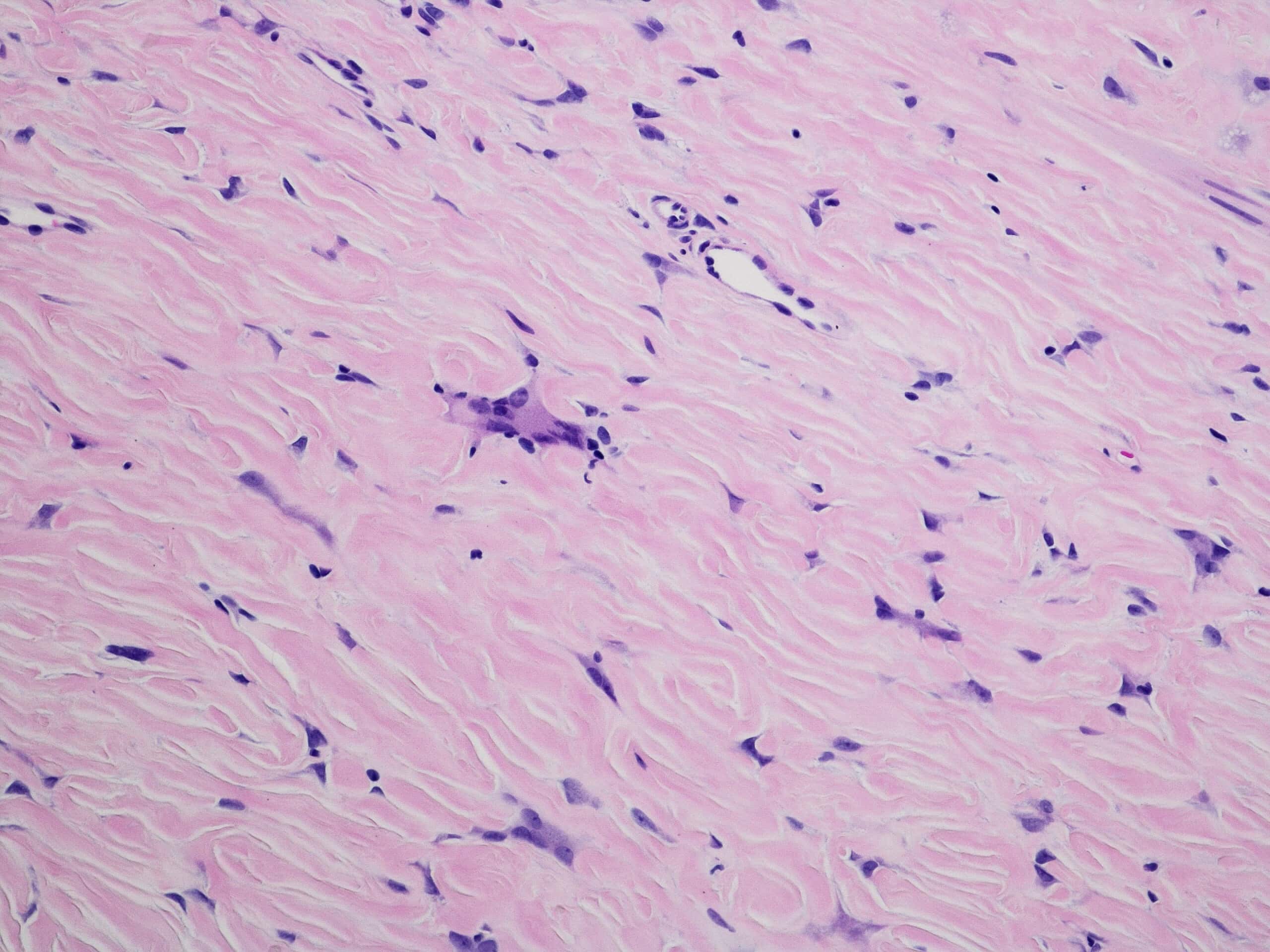
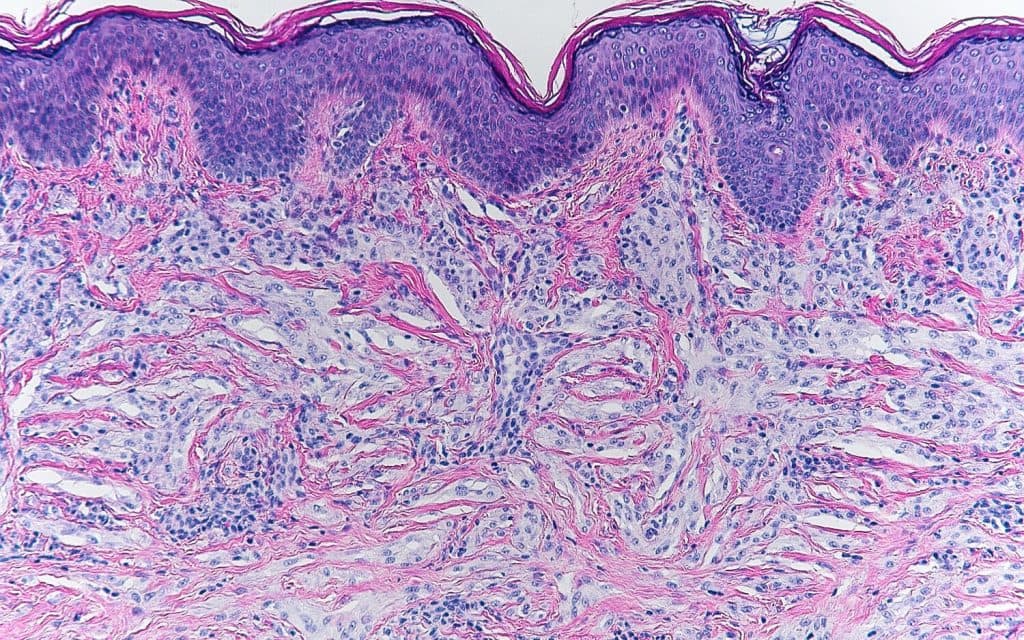
A 60-year-old male with a slowly growing asymptomatic subcutaneous nodule on the right shoulder presented to dermatology clinic for evaluation. A biopsy was done for histologic assessment. On hematoxylin & eosin (H&E) stained sections, a well circumscribed hypercellular sclerotic dermis with collagen bundles arranged in a whorled plywood pattern was appreciated (Figure 3, x100 magnification). This sclerotic collagen stroma had interspersed bizarre looking, stellate multinucleated giant cells with scant cytoplasm and plump dendritic spindle cells (Figure 4, x200 magnification). Nuclear atypia and mitotic figures were absent in multiple examined step sections. The mononucleated plump dendritic spindle cells stain with vimentin and actin HHF35 immunohistochemistry stains, whereas the multinucleated giant cells stain with vimentin only(3). Both populations of cells are negative for cytokeratin, smooth muscle actin, desmin, S-100 protein, CD34, and Factor XIIIa(1). The described features above are those of a giant cell collagenoma.
Giant cell collagenoma is a histologically distinct entity, and it is important to distinguish it from other fibrotic lesions with multinucleated giant cells. The differential diagnosis includes but is not limited to pleomorphic fibroma, atypical fibrous histiocytoma, atypical fibroxanthoma and giant cell fibroblastoma. What differentiates giant cell collagenoma from all of these entities is its well circumscribed appearance, presence of a whorled sclerotic stroma and the absence of mitotic figures and atypical nuclei. Additionally, giant cell collagenoma is differentiated from pleomorphic fibroma on immunohistochemical grounds as well: the multinucleated giant cells in pleomorphic fibroma show positivity for vimentin, actin and CD34(3), while the multinucleated giant cells in giant cell collagenoma stain for vimentin only.
While both case series that described and further expanded on the entity giant cell collagenoma(1,3) did not show a connection between giant cell collagenomas and Cowden’s syndrome, we have seen far too few of these cases to absolutely say for sure that there is no connection whatsoever. Thus, clinical correlation is recommended and quite necessary.
Hope you join me next month for another brief but exciting and educational dermatopathology article,
Kind regards,
Silvija P. Gottesman, MD, FAAD
Dermatologist/Dermatopathologist
Assistant Professor of Dermatology and Pathology
Zucker School of Medicine at Hofstra/Northwell
Twitter: @SGottesmanMD
References:
1. Rudolph P, Schubert C, Harms D, Parwaresch R. Giant cell collagenoma: a benign dermal tumor with distinctive multinucleate cells. Am J Surg Pathol. 1998;22(5):557-63.
2. Weary PE, Gorlin RJ, Gentry WC, Comer JE, Greer KE. Multiple hamartoma syndrome (Cowden’s disease). Arch Dermatol. 1972;106(5):682-90.
3. Brito H, Pereira EM, Reis-filho JS, Maeda SA. Giant cell collagenoma: case report and review of the literature. J Cutan Pathol. 2002;29(1):48-51.
{kind=link}
{kind=link}