60 Year old Man with Copious Diarrhea
May 28, 201976 year old female presenting with a slowly enlarging mass
November 3, 2019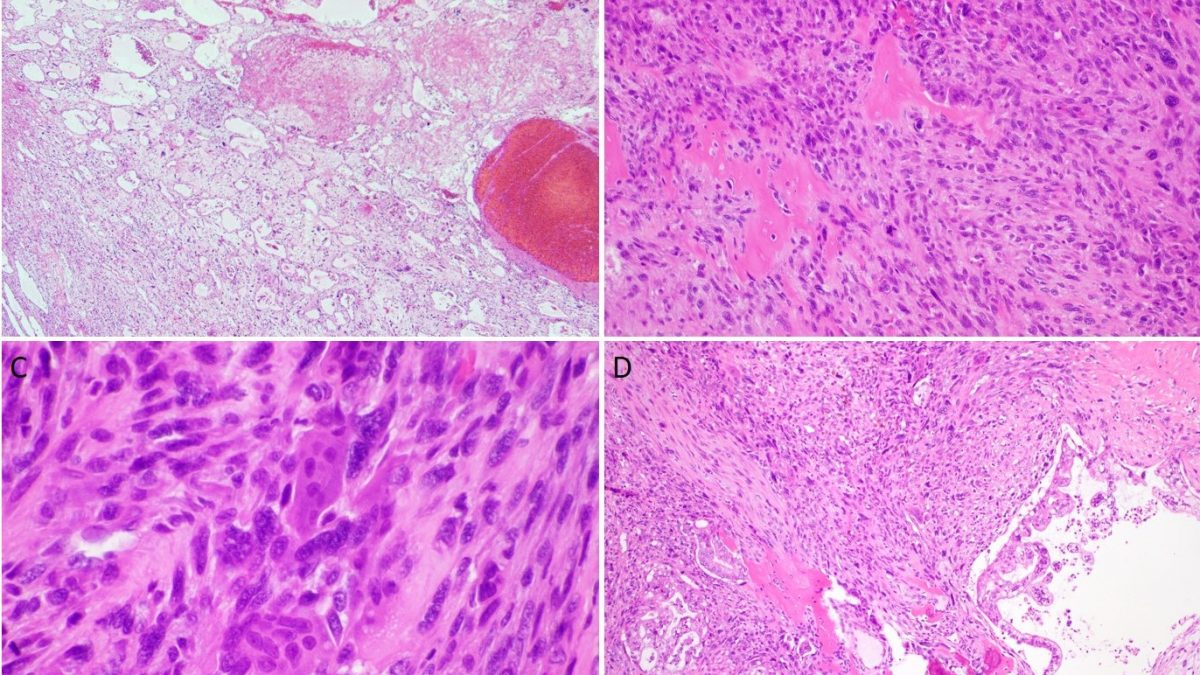
A 71-year-old male with a past medical history of a colonic GIST, presented with abdominal pain, jaundice, and a 15-20 pound weight loss over a course of few weeks. Laboratory studies revealed an elevated CA 19-9 of 142. A CT abdomen demonstrated a hyperenhancing pancreatic head mass measuring 1.7 cm in greatest dimension with pancreatic duct dilatation.
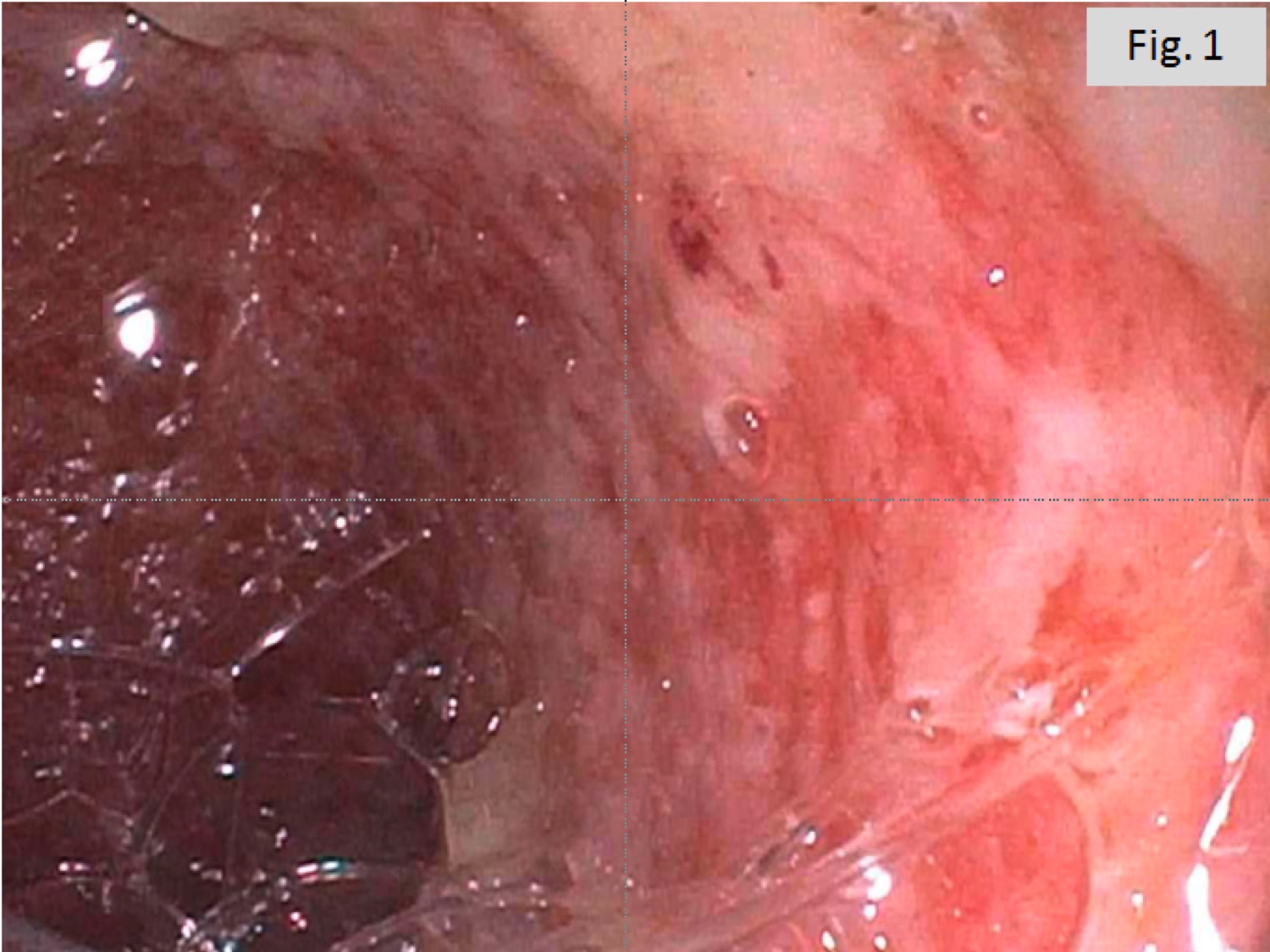
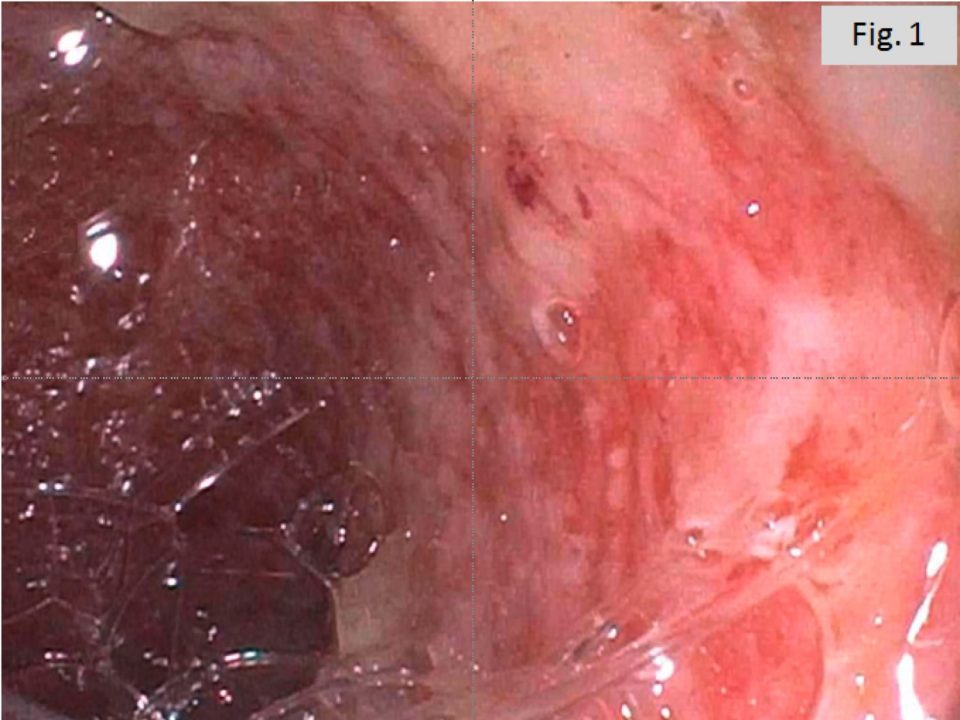
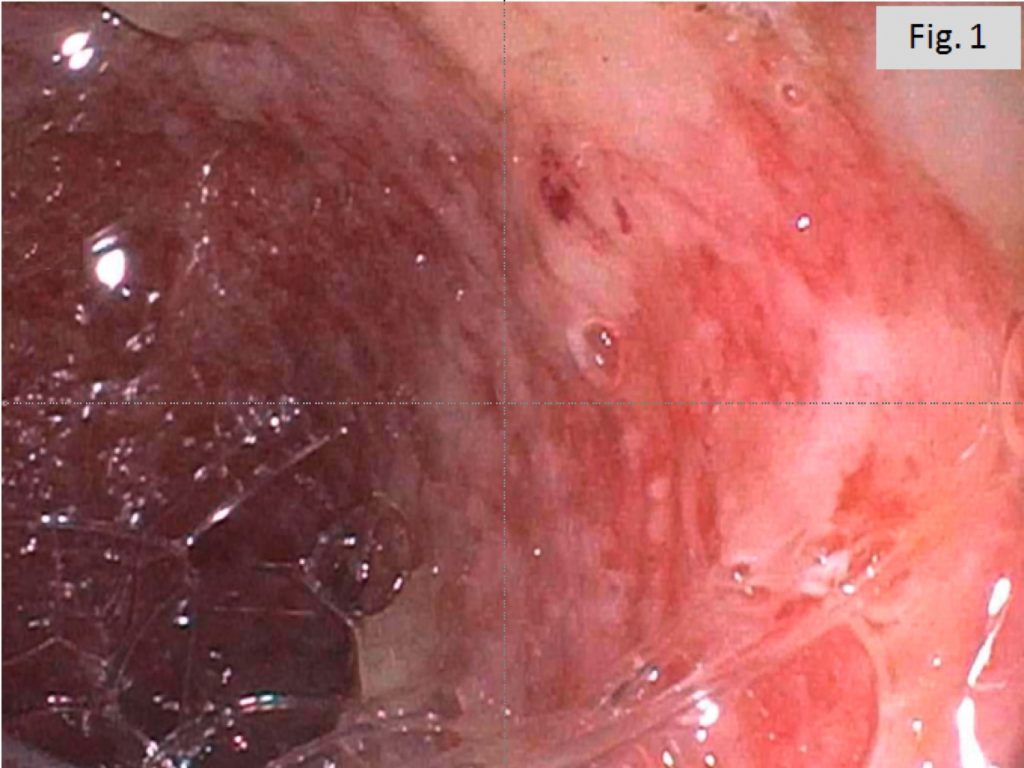
A core biopsy sample of the mass, performed at an outside institution, demonstrated a malignant spindle cell neoplasm with focal osteoid formation. Subsequently patient underwent a pancreatoduodenectomy (Whipple) procedure. Gross examination of the specimen revealed a 4.5 x 4.0 x 2.5 cm bulging, bosselated mass in the ampullary region with a tan-brown fleshy cut surface that appeared to involve the pancreatic duct (Figures 1A, B).
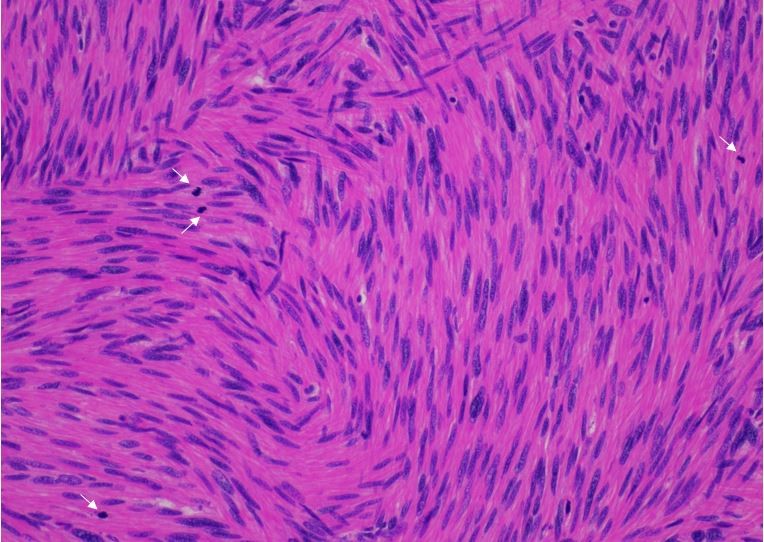
Histologic sections revealed a hypercellular malignant spindle cell neoplasm with areas of cystic degeneration and associated hemorrhage (Figure 2A). There were occasional foci of osteoid deposition (Figure 2B). Osteoclast-like giant cells with dense eosinophilic cytoplasm and multiple ovoid uniform nuclei were frequently admixed with larger mononuclear cells with hyperchromatic and irregular nuclei (Figure 2C). There were rare foci of neoplastic pancreatic glands with clear cytoplasm and enlarged, irregular nuclei characteristic of conventional pancreatic ductal adenocarcinoma (Figure 2D).
What is your diagnosis?
This is an undifferentiated carcinoma of the pancreas with osteoclast-like giant cells (UCOGC), a rare pancreatic neoplasm with a reported incidence of 1-2% of pancreatic malignancies [1]. This tumor is considered a sarcomatoid carcinoma, characterized by the presence of admixed osteoclast-like giant cells, which are CD68 positive and cytokeratin negative. These cells are in fact benign and are recruited through chemotaxis [1].
UCOGCs are thought to be epithelial in origin despite its sarcomatoid appearance as most are associated with a conventional ductal adenocarcinoma [1]. Further supporting the epithelial origin of these tumors is a recent report of whole exome sequencing of eight UCOGC cases which showed similar activating mutations to those seen in conventional pancreatic ductal adenocarcinoma (PDC) including alterations in KRAS, TP53, CDKN2A, and SMAD4 [2]. Nevertheless, there are some differences in presentation between UCOGC and conventional PDC. A third of UCOGC occurs in the body and tail of the pancreas, and it is often larger than PDC at presentation [1]. UCOGC presents a decade earlier than PDC (mean age 57.9 years vs. 65.0) and is seen more frequently in women [1]. There are mixed data on the clinical course of this entity as some studies suggest that pure UGOGC’s (i.e. those with no associated ductal component) have a higher 5-year survival than conventional PDCs (59% vs 16%) while others suggest that, if associated with a ductal adenocarcinoma component, the survival is similar to conventional PDCs [1, 2] .
While readily recognizable because of the presence of giant cells, the differential diagnosis of UCOGCs includes pancreatic undifferentiated rhabdoid carcinoma and osteosarcoma. Immunohistochemical stains are helpful in these settings as INI1 is lost in pancreatic rhabdoid carcinoma and SATB2 is positive in osteosarcomas [3].
Case submitted by Dr. Maria Mostyka of New York Presbyterian Hospital-Weill Cornell Medicine
References:
- Muraki T. Undifferentiated Carcinoma with Osteoclastic Giant Cells of the Pancreas: Clinicopathological Analysis of 38 Cases Highlights A More Protracted Clinical Course than Currently Appreciated. American Journal of Surgical Pathology. 2016;40(9):1203-1216. doi:10.1097/PAS.0000000000000689.
- Luchini C., et al. Pancreatic undifferentiated carcinoma with osteoclast-like giant cells is genetically similar to, but clinically distinct from, conventional ductal adenocarcinoma. Journal of Pathology. 2017;243:148-154. doi:10.1002/path.4941.
- Agaimy A, et al. Pancreatic undifferentiated rhabdoid carcinoma: KRAS alterations and SMARCB1 expression status define two subtypes. Modern Pathology. 2015;28:248-260. doi:10.1038/modpathol.2014.100.
Figure legends
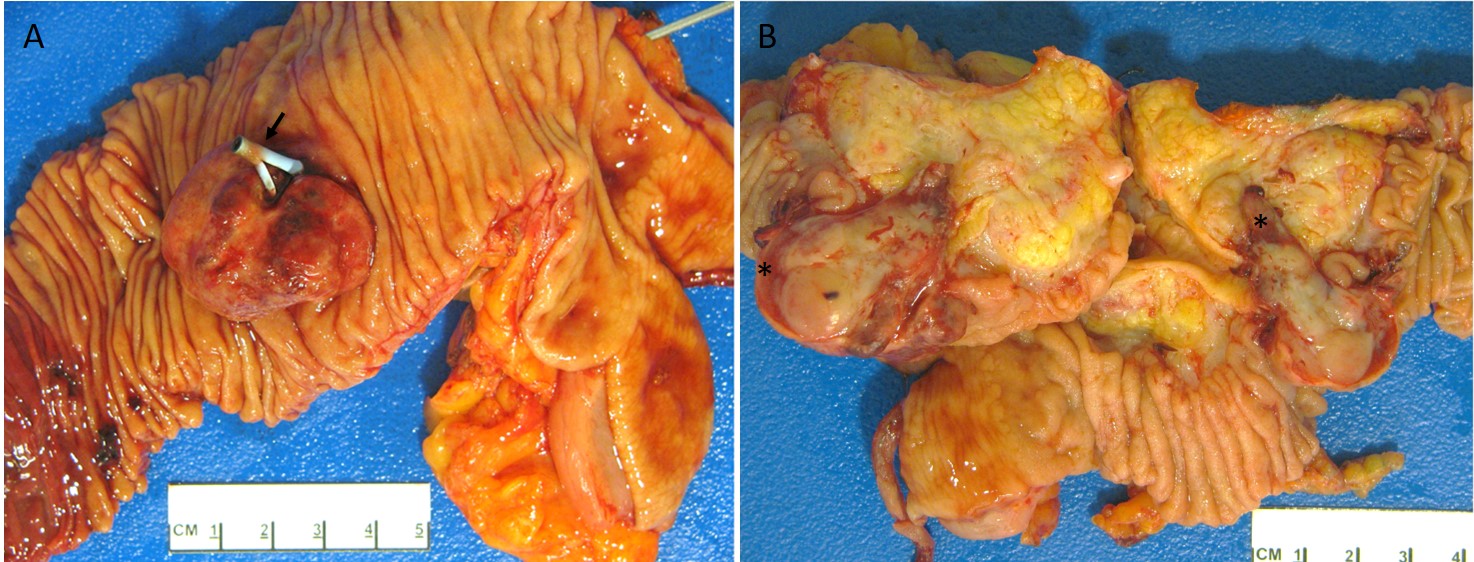
Figure 1. Opening the duodenum of the pancreatoduodenectomy specimen revealed a 4cm erythematous bulging mass at the ampulla associated with a biliary stent (arrow) (A). The mass has a tan fleshy cut surface with foci of hemorrhage and necrosis (*). It appears to arise from the pancreatic head and involve the ampulla. The remainder of the pancreas is yellow and lobulated with no other masses or lesions (B).

Figure 2. At low magnification, there are areas of cystic degeneration and hemorrhage, common in undifferentiated carcinoma of the pancreas with osteoclast-like giant cells (A). The lesion is made up of sheets of highly atypical spindle cells with large, hyperchromatic nuclei, frequent mitoses and occasional foci of osteoid deposition (B). Osteoclast-like giant cells with multiple bland nuclei are frequent (C). One section from the mass shows a small focus of conventional pancreatic ductal adenocarcinoma (D).
{kind=link}
{kind=link}